At TrueCare RCM, we provide specialized credentialing and provider enrollment solutions built for Internal Medicine practices. Whether you’re a solo provider, a growing group, or a multi-location clinic, we handle every step of your Medicare, Medicaid, and commercial payer enrollment — so you get approved faster and get paid without gaps.
Complete Credentialing & Provider Enrollment Support for Internal Medicine Practices
Internal Medicine Credentialing Services That Eliminate Enrollment Delays
✅ CAQH profile setup, maintenance & quarterly attestation
✅ Medicare PECOS enrollment — individual, group & reassignments
✅ Commercial payer credentialing — BCBS, Aetna, UHC, Cigna & more
✅ Subspecialty credentialing — cardiology, pulmonology, GI & more
✅ Weekly payer follow-up, status tracking & escalation
✅ Billing clearance notification — exact effective dates confirmed
Complete Payer Enrollment and Credentialing Support for Internal Medicine Practices
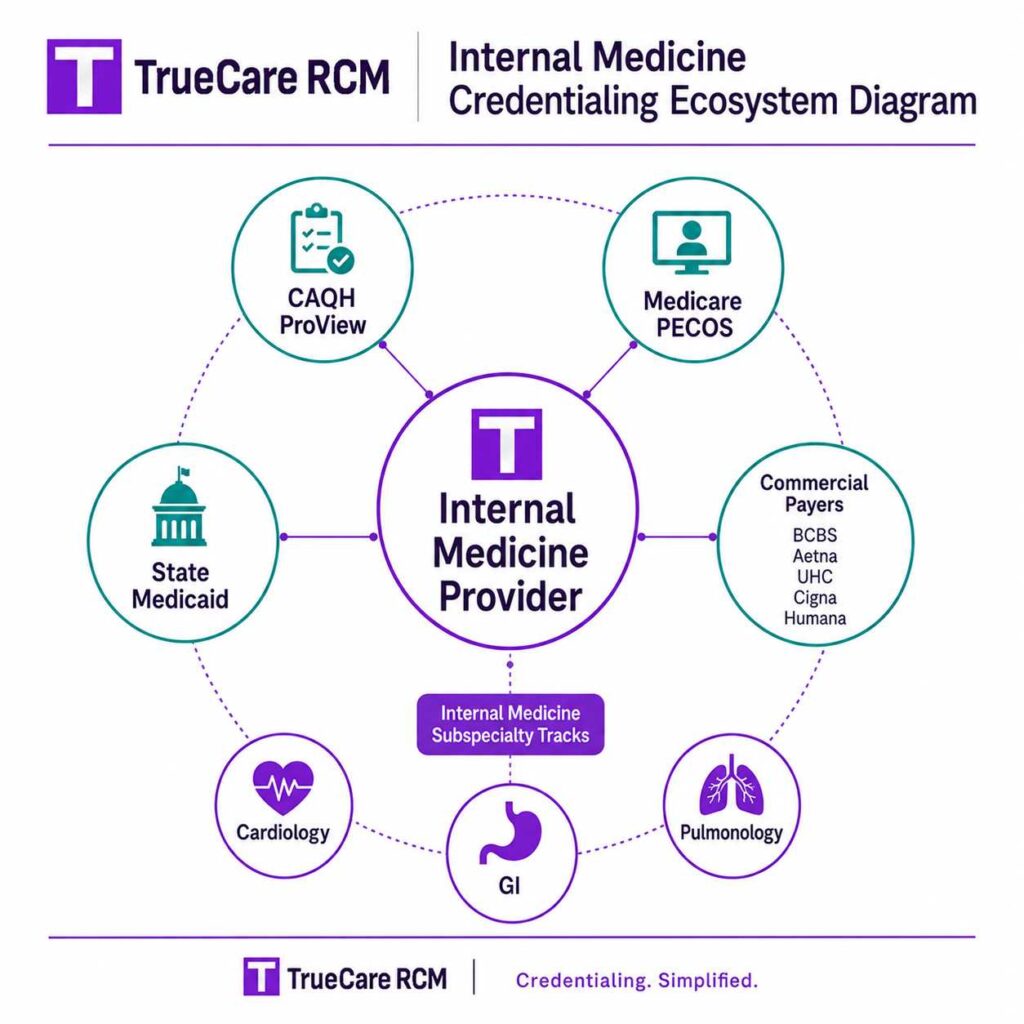
Internal medicine physicians often carry subspecialty certifications — cardiology, gastroenterology, pulmonology, endocrinology — that require separate payer credentialing tracks. Managing dual taxonomy codes, subspecialty privilege documentation, and multi-payer enrollment simultaneously is where most generic credentialing services fall short.
At TrueCare RCM, we understand the nuances of IM credentialing and track every application with specialty-level detail. Our credentialing coordinators work directly with payers on your behalf — no middlemen, no stalled queues. Whether you’re enrolling for the first time, adding a subspecialty, or onboarding a new provider to an existing group, we map every moving part before a single form goes out.
60–120 Days
Medicare & Medicaid Enrollment
45–90 Days
Commercial Payer Credentialing
100%
Dedicated Credentialing Support
Zero Revenue Gaps
With Effective Date Tracking
Nationwide Support
Credentialing Help Across Priority U.S. States
Credentialing Solutions Tailored for Internal Medicine Practices
Our credentialing services are built for the real-world needs of internal medicine providers. We support first-time enrollments, payer additions, provider onboarding, recredentialing, group practice updates, multi-location changes, ownership updates, and payer record cleanup.
✔ CAQH Profile Setup & Maintenance
Complete setup, document upload, and 120-day re-attestation management so your profile never lapses and stalls an active application.
✔ Medicare PECOS Enrollment
Individual and group PECOS enrollment, reassignment filings, and EFT setup for clean Medicare billing from day one.
✔ Commercial Payer Applications
BCBS, Aetna, UHC, Cigna, and regional payers — each tracked independently with weekly follow-up calls and escalation when applications stall.
✔ Subspecialty Credentialing
Separate credentialing tracks for board-certified subspecialties including cardiology, gastroenterology, pulmonology, and endocrinology — with correct dual taxonomy codes and payer-specific documentation for each.
✔ Medicaid State Enrollment
All-state Medicaid credentialing with state-specific knowledge of requirements, processing timelines, and re-enrollment cycles.
✔ NP/PA Mid-Level Credentialing
Enrollment of physician assistants and nurse practitioners under appropriate supervision structures at every payer — with attention to state-specific scope-of-practice rules.
✔ Recredentialing & Revalidation
Proactive 3-year recredentialing cycle tracking so your IM practice never loses network status with Medicare, Medicaid, or commercial payers.
✔ Denial & Appeal Management
Application rejections reviewed, corrected, and resubmitted with root cause documentation — no rejection sits unaddressed.
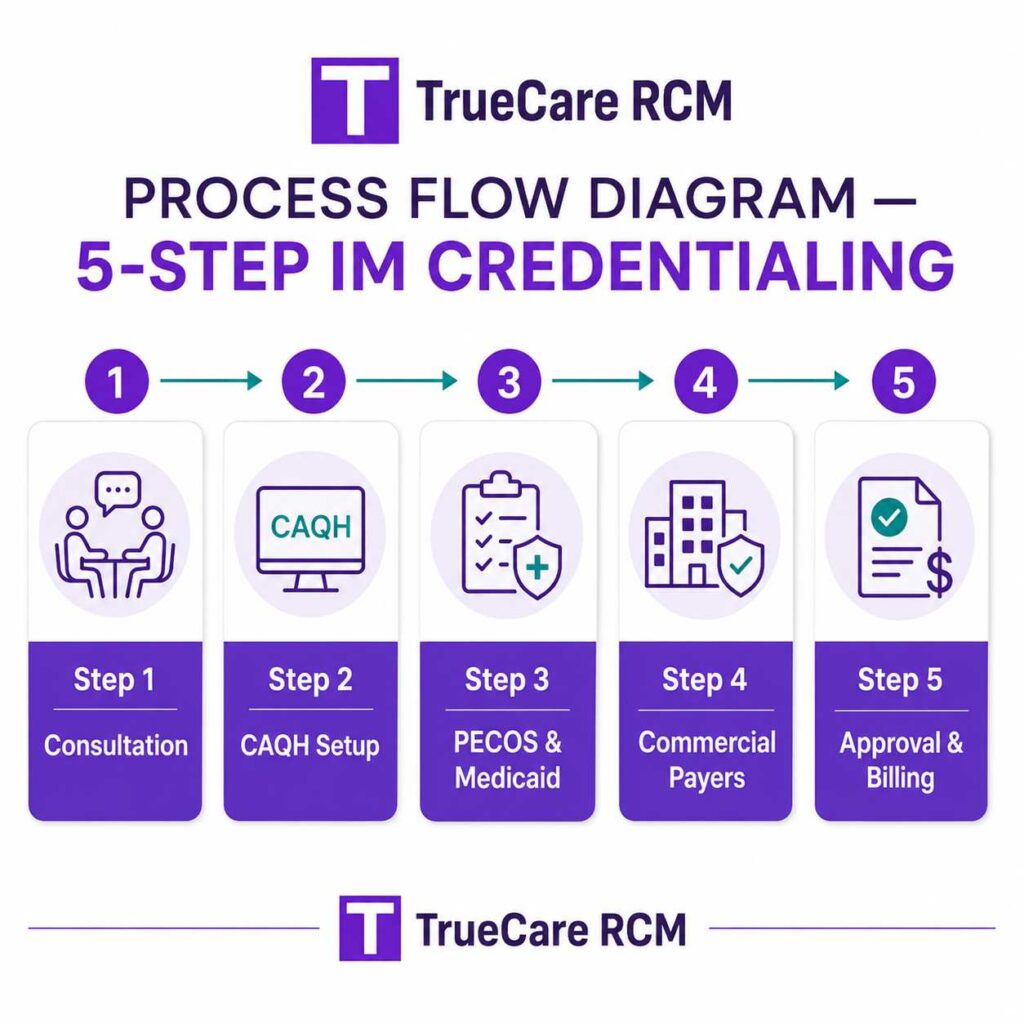
Our Internal Medicine Credentialing Process – Step by Step
We do not simply submit applications and wait. Our process is structured, tracked, and designed to keep your internal medicine practice informed throughout the credentialing lifecycle.
- CAQH profile setup and payer-specific document preparation
- PECOS Medicare enrollment and Medicaid state applications
- Commercial payer credentialing and payer panel follow-up
- NPI, taxonomy, group enrollment, and reassignment review
- Real-time status tracking and escalation for delayed applications
- Approval confirmation and billing activation support
Step – 01
Step – 02
Step – 03
Step – 04
Step – 05
How Long Internal Medicine Credentialing Takes – Realistic Timelines
One of the most common questions we hear from IM practices: ‘How long is this actually going to take?’ The honest answer depends on payer type, state, and complexity. Here’s what to realistically plan for:
| Payer Type | Typical Timeline | Notes |
| Medicare (PECOS) | 60–120 days | High-demand states (CA, NY, TX) typically run longer; new enrollments trend toward the upper end |
| Medicaid | 60–120 days | State-specific variation — some programs require 90+ days; concurrent filing saves time where possible |
| Commercial Payers | 45–90 days | Dependent on CAQH completeness and current payer backlog at BCBS, Aetna, UHC, and Cigna |
| Subspecialty Credentialing | 60–120 days | Additional documentation review for cardiology, GI, and pulmonology adds complexity and review time |
| CAQH Attestation Cycle | 30–45 days | Re-attest every 120 days — a lapsed profile stalls all active applications simultaneously |
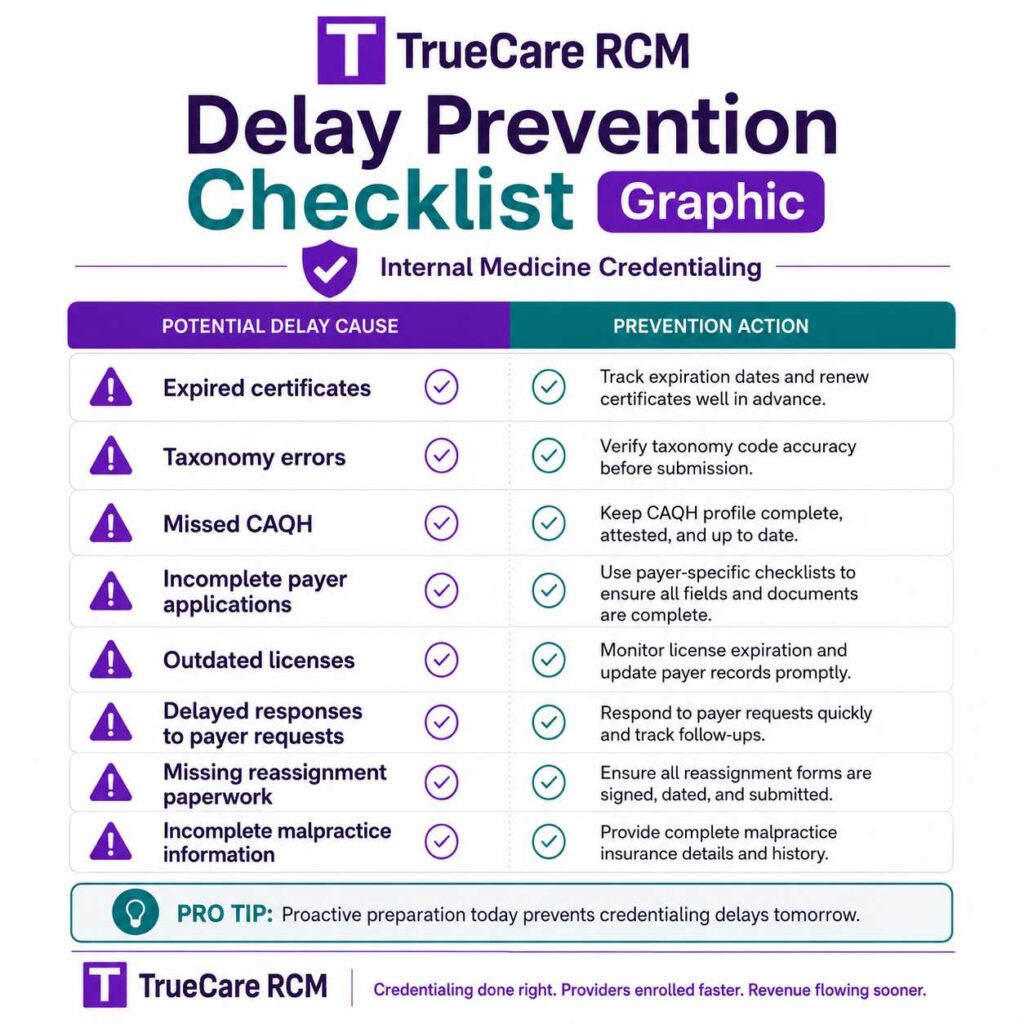
Common Internal Medicine Credentialing Delays — And How We Prevent Them
Most credentialing delays are preventable. They’re caused by small, fixable mistakes — a missed document, a wrong taxonomy code, an expired certificate nobody was tracking. Here’s what typically derails IM practices, and exactly what we do about it:
| Common Delay | How TrueCare RCM Prevents It |
| Missing subspecialty documentation | All board certifications and fellowship records uploaded before submission — nothing filed until the file is complete |
| Incorrect dual taxonomy codes | Primary and subspecialty taxonomy codes verified against each payer’s requirements before every filing |
| Expired malpractice or DEA certificates | Expiration dates tracked; renewals flagged proactively before any payer notices the gap |
| NPI mismatches between individual and group | NPPES cross-check completed before filing any PECOS or commercial application |
| Missed CAQH re-attestation | Attestation calendar owned and managed — re-attestation completed every 120 days without prompting |
| Stalled applications in high-demand states | Weekly follow-up and escalation to dedicated payer contacts — no application sits idle for more than 7 days |
| NP/PA supervision structure errors | State-specific supervision requirements verified per payer before any mid-level application is filed |
Who We Serve in Internal Medicine Credentialing
Our internal medicine credentialing services aren’t built for one type of practice. We support the full range of IM providers — from solo internists starting fresh to large multi-specialty groups adding subspecialty tracks.
| Practice Type | How We Help |
| Solo Internists | Complete enrollment from scratch across all payers — ideal for physicians transitioning from hospital employment to independent practice |
| Multi-Provider IM Groups | Each provider’s credentialing tracked independently across shared and separate payer panels, with group-level coordination |
| Subspecialty IM Physicians | Separate credentialing tracks for cardiologists, gastroenterologists, pulmonologists, and endocrinologists practicing under an IM group |
| Hospitalists & Teaching Physicians | Facility and professional credentialing coordinated for hospital-based IM providers, including institutional privilege verification where required |
| NP/PA Internal Medicine Providers | Mid-level credentialing filed under the correct supervision structure at every payer, with state-specific scope-of-practice compliance |
| New Practice Startups | First-time enrollment from zero — we build your credentialing file and guide you through every payer’s requirements from day one |
Frequently Asked Questions About Internal Medicine Credentialing Services
Everything your practice needs to know about IM credentialing — answered directly.
Internal medicine credentialing services manage the formal process of verifying a provider’s qualifications with insurance payers so they can bill for services. This includes CAQH profile setup, Medicare PECOS enrollment, Medicaid applications, and commercial payer credentialing with BCBS, Aetna, UHC, Cigna, and others. For IM practices, it also covers subspecialty credentialing tracks for cardiologists, gastroenterologists, and pulmonologists practicing under the same group.
Payers require credentialing to verify that a provider meets their standards for licensure, training, board certification, and malpractice coverage before agreeing to reimburse their services. Without approved credentialing, claims submitted to Medicare, Medicaid, or commercial insurers will be denied — or paid back retroactively to the enrollment effective date in some cases. Credentialing is not optional; it’s the gateway to getting paid.
Medicare (PECOS) typically takes 60–120 days. Medicaid timelines vary by state but generally fall in the same range. Commercial payers like BCBS, Aetna, UHC, and Cigna average 45–90 days depending on current payer backlog and how complete your CAQH profile is. Subspecialty credentialing often runs 60–120 days due to additional documentation review. TrueCare RCM gives you realistic timelines upfront and actively compresses them through weekly payer follow-up.
Every IM credentialing application requires: MD or DO degree certificate, residency completion certificate, board certification (ABIM), current state medical license, DEA registration, malpractice insurance certificate, NPI (individual and group), and EIN for groups, with a complete CAQH profile. Subspecialty credentialing adds fellowship or additional board certification documentation. We collect, verify, and track every document before filing.
Yes — CAQH ProView is the foundation of commercial payer credentialing. More than 1,400 insurance companies pull your credentials directly from CAQH. Providers must re-attest every 120 days to keep the profile active. If re-attestation is missed, payers cannot access your file and any active credentialing applications stall. TrueCare RCM manages your CAQH setup and ongoing maintenance — including re-attestation — as part of our service.
Credentialing is the verification process — confirming your education, training, licensure, and malpractice history. Payer enrollment is the contracting step — where you’re added to a payer’s network and authorized to bill them. You typically must complete credentialing before payer enrollment is finalized. TrueCare RCM manages both steps simultaneously to reduce overall timelines.
No — not directly. You can see patients on a self-pay or cash basis while credentialing is pending, or provide superbills for patients to submit for out-of-network reimbursement. But submitting claims to insurers before credentialing is approved will result in denials. TrueCare RCM confirms the exact effective date for each payer and notifies your billing team when it’s safe to submit.
Yes. NPs and PAs must be individually credentialed with each payer they bill under. Requirements vary by payer and state — some require independent enrollment, others require a supervising physician relationship to be documented. TrueCare RCM handles NP and PA credentialing under the correct supervision structure for every payer, ensuring compliance and preventing claim denials.
Yes. If multiple providers bill under a shared Tax Identification Number (TIN), the group itself must be enrolled separately — and individual providers must file PECOS reassignments so Medicare payments route correctly to the group. Many groups overlook this step, which causes payment delays or misdirected reimbursements. We handle individual enrollment, group enrollment, and all reassignment filings in a coordinated sequence.
Absolutely. Medicare PECOS enrollment and Medicaid state enrollment are core components of every credentialing engagement we manage. For internal medicine practices — especially those serving elderly or underinsured populations — Medicare and Medicaid credentialing is often the highest priority. We file both simultaneously wherever possible and track them through to effective date confirmation.
At minimum: Medicare, Medicaid (in your state), and the major commercial payers in your market — BCBS, Aetna, UHC, Cigna, and Humana. Beyond that, the right payer mix depends on your patient population, location, and whether you participate in value-based care contracts. TrueCare RCM conducts a payer mapping consultation as the first step to identify which payers matter most for your specific practice.
Most payers require recredentialing every two to three years. Medicare revalidation is typically required every five years for low-risk providers. Missing a recredentialing deadline can result in termination from the network, which means revenue stops until re-enrollment is complete. TrueCare RCM tracks all recredentialing cycles proactively and initiates the process well before any deadline.
The most common causes are: incomplete CAQH profiles, incorrect or missing taxonomy codes (especially for subspecialties), expired malpractice or DEA certificates, NPI mismatches between individual and group records, missed CAQH re-attestation, and lack of proactive follow-up with payers. All of these are preventable — see our delay prevention table above for the exact steps we take to eliminate each one.
Every day you’re not credentialed is a day you can’t bill insurance. For a solo internist, that can mean $500–$2,000+ in missed revenue per day. For a multi-provider IM group, the number compounds quickly. Beyond lost billing revenue, delays in onboarding new providers or subspecialists can force you to turn away patients — or refer them elsewhere permanently. Fast, clean credentialing protects your revenue from the moment a new provider joins.
Credentialing is one of the most time-intensive administrative tasks in a medical practice. Between CAQH maintenance, payer applications, weekly follow-up calls, and tracking effective dates across a dozen payers, in-house management easily consumes 10–20 hours per provider enrollment. Outsourcing to TrueCare RCM transfers all of that to a dedicated specialist — so your office staff focuses on patient care, not payer phone queues.
Get Started with Internal Medicine Credentialing Today
Avoid enrollment delays, protect your revenue, and get in-network faster with TrueCare RCM. Our dedicated credentialing team manages every step — from CAQH setup to billing activation — so you can focus on your patients while we handle the paperwork.
Contact us today for a free credentialing consultation.
From CAQH and PECOS to Medicare, Medicaid, Medicare Advantage, commercial payers, recredentialing, and billing activation, our team manages the details so your practice can focus on patient care.

Why Internal Medicine Credentialing Matters for Practice Revenue
Internal medicine is one of the highest-volume specialties in primary care — which means your payer relationships determine your revenue more directly than almost any other factor in your practice. Every uncredentialed payer is a patient population you can’t bill. Every delayed enrollment is days — sometimes weeks — of missed claims. And in a specialty where patient volume is high and margins are tight, those gaps compound fast.
Internal medicine practices typically need to be in-network with every major commercial payer in their market — plus Medicare and Medicaid. That’s often 10–15 separate credentialing applications per provider. Managing that volume in-house is a full-time job. Outsourcing to TrueCare RCM means all 10–15 applications run in parallel, tracked weekly, with escalation when anything stalls.
NPs and PAs are increasingly central to internal medicine delivery — especially in high-volume primary care settings. Each mid-level provider needs independent credentialing with every payer they bill under, and supervision requirements vary by state and payer. Getting this wrong means claim denials that are difficult to recover. Getting it right means your NPs and PAs are revenue-generating from their first day.
The standard taxonomy for general internal medicine is 207R00000X. Subspecialties carry their own codes — 207RC0000X for cardiovascular disease, 207RG0100X for gastroenterology, and so on. Filing the wrong code — or omitting a subspecialty code — can result in credentialing denial or misdirected claims. We verify every code against every payer’s current requirements before any application is submitted.
More than 1,400 commercial insurers pull credentials directly from CAQH ProView. A complete, up-to-date profile accelerates every commercial payer application. A stale or incomplete profile stalls them all. For internal medicine practices with multiple providers and subspecialties, CAQH management alone can become a part-time responsibility. TrueCare RCM owns your CAQH calendar — setup, updates, and re-attestation every 120 days.
If your internal medicine group has 10 or more providers, you may qualify for delegated credentialing arrangements with certain payers — which can dramatically accelerate enrollment timelines. TrueCare RCM can evaluate whether your group qualifies and manage the delegation agreement process on your behalf.
Every new physician, NP, or PA joining your IM group needs to go through credentialing before they can bill. The sooner you start, the sooner they’re productive. TrueCare RCM builds a credentialing workflow that integrates with your hiring timeline — so new provider onboarding doesn’t become a revenue bottleneck.
Internal Medicine Credentialing Documentation Checklist
Before a single application leaves our office, every document needs to be in place. Here’s the full checklist we work through for every internal medicine provider we credential:
Core Credentials
- MD or DO degree certificate
- Residency completion certificate (ACGME-accredited internal medicine program)
- Board certification — American Board of Internal Medicine (ABIM)
- Fellowship certificates for any subspecialty (cardiology, GI, pulmonology, endocrinology)
Licensing & Registrations
- Current state medical license (in every state where you practice)
- DEA (Drug Enforcement Administration) registration certificate
- NPI — both individual (Type 1) and group (Type 2) if applicable
- EIN (Employer Identification Number) for group billing
Insurance & Compliance
- Malpractice insurance certificate (typically $1M/$3M minimum coverage)
- Tail coverage documentation if transitioning from a previous employer
- OIG exclusion check clearance
- NPDB (National Practitioner Data Bank) query
Subspecialty-Specific (Cardiology, GI, Pulmonology, Endocrinology)
- Subspecialty board certification (ABIM subspecialty exam)
- Fellowship training completion documentation
- Additional taxonomy code documentation per payer requirements
- Facility credentialing documentation (for hospital-based procedures)
Internal Medicine Credentialing Glossary — Key Terms Explained
| Term | Definition |
| CAQH ProView | Universal credentialing database used by 1,400+ insurers. Providers must re-attest credentials every 120 days to keep the profile active and accessible to payers. |
| PECOS | Provider Enrollment, Chain and Ownership System — the CMS online enrollment system required for Medicare participation. IM physicians must enroll both individually and as part of any group practice. |
| NPI (National Provider Identifier) | A unique 10-digit identifier for healthcare providers. Type 1 is for individual providers; Type 2 is for organizations or groups. Both are required for group billing. |
| Taxonomy Code | A code identifying a provider’s specialty and practice type. IM providers with subspecialties may need both a primary (207R00000X) and secondary subspecialty taxonomy filed correctly at each payer. |
| ABIM | American Board of Internal Medicine — the certifying body for IM physicians and subspecialists. Board certification is required by virtually all payers as part of credentialing. |
| Reassignment (PECOS) | A process where an individual provider reassigns their right to receive Medicare payments to a group or organization. Must be filed correctly for group billing to work. |
| Recredentialing / Revalidation | The process of re-verifying provider credentials with a payer — typically every 2–3 years for commercial payers, every 5 years for Medicare. Missing this deadline can result in network removal. |
| NPDB | National Practitioner Data Bank — a federal database queried during credentialing that contains malpractice payment history, adverse actions, and licensure discipline records. |
| Delegated Credentialing | An arrangement where a large health system or MSO conducts credentialing on behalf of providers within their network, using payer-approved delegation agreements. |
| EFT (Electronic Funds Transfer) | Setup required during PECOS enrollment to direct Medicare reimbursements to the correct bank account. A missing EFT setup delays all Medicare payments even after credentialing is approved. |
| Superbill | A detailed invoice given to patients when a provider is not yet credentialed or is out-of-network. Patients submit this to their insurer for possible out-of-network reimbursement. |
| Dual Taxonomy Code | When an IM physician holds subspecialty certification, two taxonomy codes may be required — one for internal medicine and one for the subspecialty (e.g., cardiology, gastroenterology). Filing the wrong or incomplete codes is a leading cause of credentialing denials. |