At TrueCare RCM, we provide specialized credentialing and provider enrollment solutions built for emergency medicine physicians and hospital-based emergency department groups. Whether you’re a solo locum tenens emergency physician, a growing emergency medicine group, or a hospital contracted staffing organization, we handle every step of your Medicare, Medicaid, commercial payer enrollment, and hospital privileging — so you get approved faster and get paid without gaps.
Complete Payer Enrollment & Credentialing Support for Emergency Medicine Physicians and Groups
Emergency Medicine Credentialing Services Built for Fast-Moving ER Staffing
What’s included:
✅ CAQH profile setup, maintenance & quarterly attestation
✅ Medicare PECOS enrollment — individual, group & reassignments
✅ Commercial payer credentialing — BCBS, Aetna, UHC, Cigna & more
✅ Hospital medical staff privileging coordination for ED physicians
✅ Rapid onboarding support for high-turnover emergency medicine staffing
✅ Weekly payer follow-up, status tracking & escalation
Complete Payer Enrollment and Credentialing Support for Emergency Medicine Groups
Emergency medicine credentialing operates under unique pressure: ER staffing models often involve high physician turnover, locum tenens coverage, and the need for hospital medical staff privileging on top of standard payer credentialing — all while patients are being seen and billed from day one of clinical coverage, regardless of where credentialing stands.
At TrueCare RCM, we understand this urgency. Our credentialing coordinators work directly with payers and hospital medical staff offices on your behalf, prioritizing speed without sacrificing accuracy — because in emergency medicine, a credentialing delay doesn’t just cost revenue, it can mean a physician seeing a full ED shift of patients with no corresponding in-network reimbursement.
60–120 Days
Medicare & Medicaid Enrollment
45–90 Days
Commercial Payer Credentialing
100%
Dedicated Credentialing Support
Zero Revenue Gaps
With Effective Date Tracking
Nationwide Support
Credentialing Help Across Priority U.S. States
Credentialing Solutions Tailored for Emergency Medicine Physicians and Groups
Our credentialing services are built for the realities of emergency medicine — high physician turnover, hospital-based privileging requirements, and the need to move fast without cutting corners.
✔ CAQH Profile Setup & Maintenance
Complete setup, document upload, and 120-day re-attestation management so your profile never lapses and stalls an active application.
✔ Medicare PECOS Enrollment
Individual and group PECOS enrollment, reassignment filings, and EFT setup for clean Medicare billing from day one.
✔ Commercial Payer Applications
BCBS, Aetna, UHC, Cigna, and regional payers — each tracked independently with weekly follow-up calls and escalation when applications stall.
✔ Hospital Medical Staff Privileging
Coordination of medical staff privileging applications required for emergency physicians to practice within a specific hospital’s emergency department, run in parallel with payer credentialing.
✔ Rapid Onboarding for High-Turnover Staffing
Streamlined intake and document collection processes designed for the fast-moving reality of ER staffing groups, where new physicians join coverage rotations frequently.
✔ NP/PA Emergency Medicine Credentialing
Enrollment of nurse practitioners and physician assistants working in emergency and urgent care settings, under appropriate supervision structures at every payer.
✔ Recredentialing & Revalidation
Proactive 3-year recredentialing cycle tracking so your emergency medicine group never loses network status with Medicare, Medicaid, or commercial payers.
✔ Denial & Appeal Management
Application rejections reviewed, corrected, and resubmitted with root cause documentation — no rejection sits unaddressed.
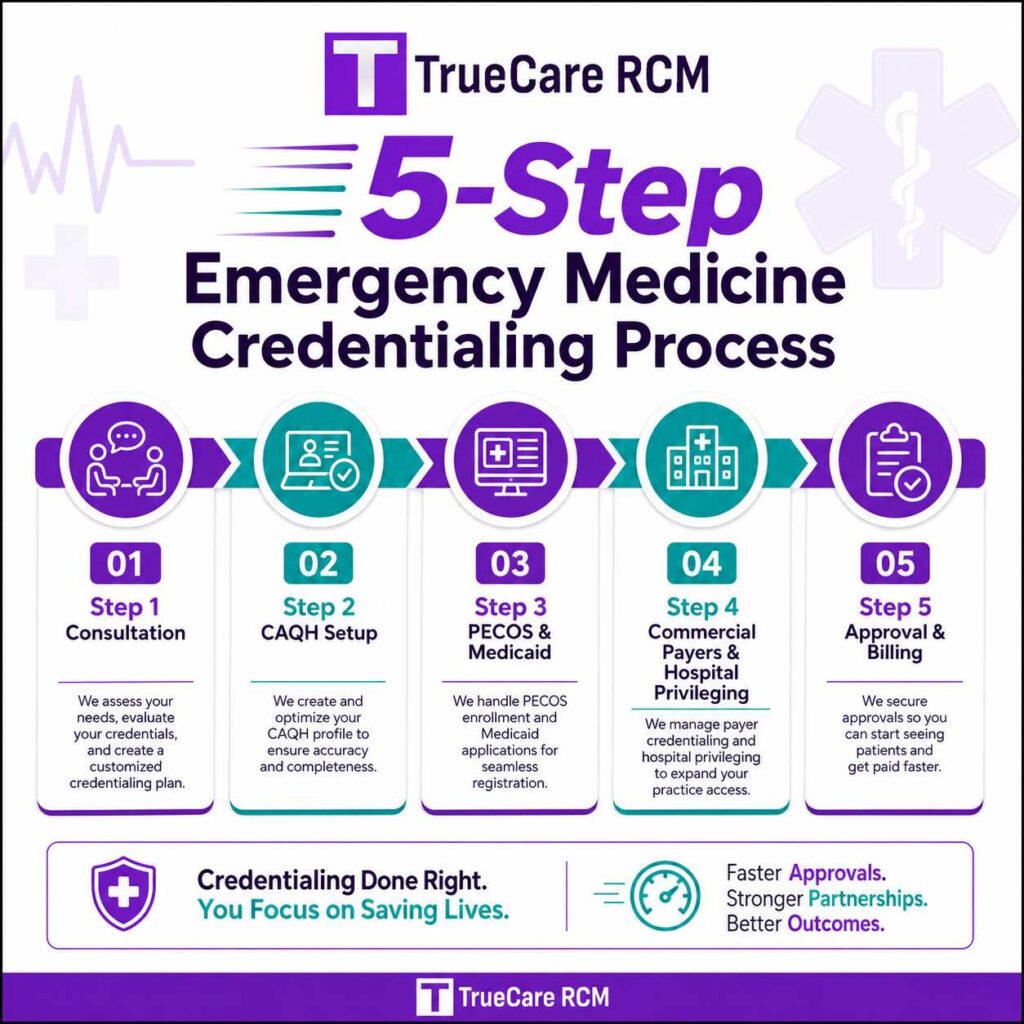
Our Emergency Medicine Credentialing Process — Step by Step
We do not simply submit applications and wait. Our process is structured, tracked, and built for speed — because in emergency medicine, every day of delay is a day of unbillable shifts.
- CAQH profile setup and payer-specific document preparation
- PECOS Medicare enrollment and Medicaid state applications
- Commercial payer credentialing and payer panel follow-up
- Hospital medical staff privileging coordination
- Real-time status tracking and escalation for delayed applications
- Approval confirmation and billing activation support
Step – 01
Step – 02
Step – 03
Step – 04
Step – 05
How Long Emergency Medicine Credentialing Takes — Realistic Timelines
Credentialing timelines for emergency medicine depend on payer type and whether hospital privileging is involved. Here’s what to realistically plan for:
| Payer / Process | Typical Timeline | Notes |
| Medicare (PECOS) | 60–120 days | High-demand states (CA, NY, TX) typically run longer; MAC backlog adds delay |
| Medicaid | 60–120 days | State-specific variation — some programs require 90+ days |
| Commercial Payers | 45–90 days | Dependent on CAQH completeness and current payer backlog |
| Hospital Medical Staff Privileging | 60–120 days | Medical staff committee review timeline runs separately from payer credentialing |
| CAQH Attestation Cycle | 30–45 days | Re-attest every 120 days — lapses stall all active applications |
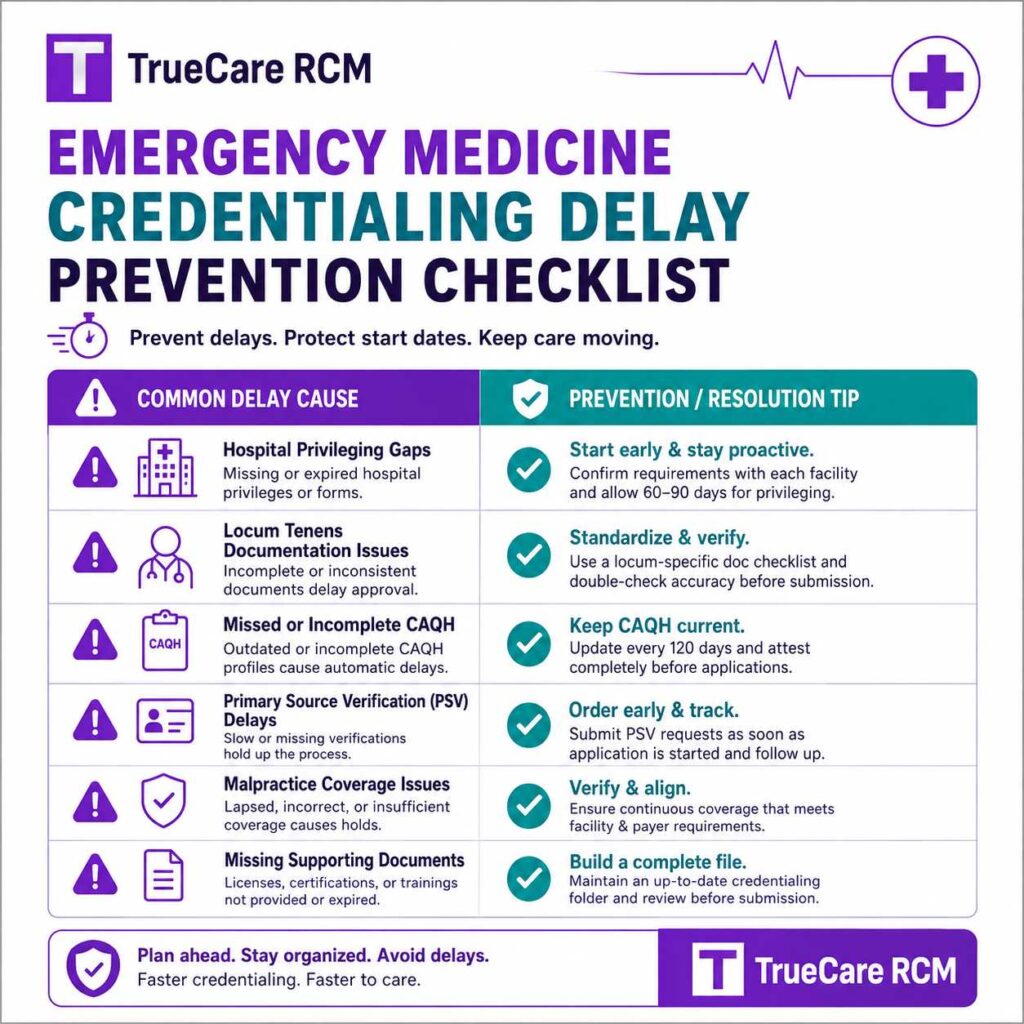
Common Emergency Medicine Credentialing Delays — And How We Prevent Them
Most delays are preventable. Here’s what typically derails emergency medicine credentialing, and exactly what we do about it:
| Common Delay | How TrueCare RCM Prevents It |
| Physician begins ED shifts before hospital privileging is approved | We track privileging status alongside payer credentialing and flag exactly when a physician is fully cleared to bill in-network |
| Locum tenens documentation incomplete or inconsistent across assignments | We maintain a current, reusable credentialing file for locum and traveling emergency physicians to speed up each new assignment |
| Incorrect taxonomy codes for emergency medicine | Taxonomy codes verified against each payer’s requirements before every filing |
| Expired malpractice or DEA certificates | Expiration dates tracked; renewals flagged proactively before any payer notices the gap |
| Missed CAQH re-attestation | Attestation calendar owned and managed — re-attestation completed every 120 days without prompting |
| NP/PA supervision structure errors in emergency or urgent care settings | State-specific supervision requirements verified per payer before any mid-level application is filed |
| Stalled applications during high physician turnover | Weekly follow-up and escalation to dedicated payer contacts — no application sits idle for more than 7 days |
Who We Serve in Emergency Medicine
Our emergency medicine credentialing services support the full range of ER staffing models — from solo locum tenens physicians to large hospital-contracted staffing groups.
| Practice Type | How We Help |
| Solo Emergency Physicians | Complete enrollment from scratch across Medicare, Medicaid, and commercial payers |
| Locum Tenens & Traveling Physicians | Reusable, well-maintained credentialing files that speed up enrollment for each new assignment |
| Hospital-Contracted ED Staffing Groups | Multi-physician credentialing and hospital privileging coordinated at scale across rotating coverage schedules |
| Multi-Site Emergency Medicine Groups | Each location’s payer and hospital privileging requirements tracked independently |
| NP/PA Emergency & Urgent Care Providers | Mid-level credentialing filed under the correct supervision structure and taxonomy at every payer |
| New Emergency Medicine Practice Startups | First-time enrollment and privileging coordination built from zero |
FAQ’s About Emergency Medicine Credentialing
Everything emergency medicine physicians and groups need to know about credentialing — answered directly.
Emergency medicine credentialing services manage the formal process of verifying an emergency physician’s qualifications with insurance payers and hospitals so they can bill for services and practice within a hospital’s emergency department. This includes CAQH profile setup, Medicare PECOS enrollment, Medicaid applications, commercial payer credentialing, and hospital medical staff privileging.
Payers require credentialing to verify a provider’s licensure, training, board certification, and malpractice coverage before agreeing to reimburse services. Without approved credentialing, claims submitted to Medicare, Medicaid, or commercial insurers will be denied — even if the physician has hospital privileges to see patients.
Medicare (PECOS) and Medicaid typically take 60–120 days. Commercial payers average 45–90 days. Hospital medical staff privileging — a separate process from payer credentialing — typically runs 60–120 days through the hospital’s medical staff committee.
Emergency medicine credentialing requires: MD or DO degree certificate, residency completion certificate, board certification (American Board of Emergency Medicine), state medical license, DEA registration, malpractice insurance certificate, and a complete CAQH profile.
Yes. CAQH ProView is used by 1,400+ insurers as the foundation for commercial payer credentialing. Profiles must be re-attested every 120 days to remain active — critical for emergency physicians who may need to credential quickly with new payers as staffing assignments change.
Credentialing is the verification process confirming a provider’s qualifications. Payer enrollment is the broader contracting process that registers the provider in the payer’s claims system so claims can be processed and paid. Hospital privileging is a separate, third process specific to practicing within a given facility.
No. Claims submitted before credentialing approval will be denied. This is especially risky in emergency medicine, where a physician may begin seeing patients under hospital privileges before payer credentialing catches up — creating a real revenue gap that’s difficult to recover retroactively.
Yes. Beyond standard payer credentialing, emergency physicians need hospital medical staff privileging to practice within a specific facility’s emergency department. This is a separate process managed by the hospital’s credentialing committee with its own documentation requirements and timeline.
Yes. NPs and PAs working in emergency or urgent care settings require their own NPI registration, taxonomy codes, and payer enrollment, along with documentation of the supervising or collaborating physician relationship required by many payers.
Yes. If multiple physicians bill under a shared Tax ID — common in hospital-contracted ED staffing groups — the group itself must be enrolled separately, and individual providers must file reassignment of benefits so payments route correctly.
Absolutely. Medicare PECOS enrollment and Medicaid state enrollment are core components of every credentialing engagement we manage for emergency medicine physicians and groups.
At minimum: Medicare, Medicaid, and the major commercial payers active in the hospital’s service area — BCBS, Aetna, UHC, and Cigna. Because emergency departments see patients regardless of insurance status, broad payer participation is typically necessary.
Most commercial payers require recredentialing every 2–3 years. Medicare revalidation is typically required every 5 years. CAQH profiles must be re-attested every 120 days — particularly important for physicians moving between staffing assignments frequently.
Common causes include physicians beginning ED shifts before hospital privileging is approved, incomplete or inconsistent locum tenens documentation, incorrect taxonomy codes, expired malpractice or DEA certificates, and missed CAQH re-attestation.
Emergency medicine staffing moves fast, with frequent physician turnover and dual-track requirements (payer credentialing plus hospital privileging). Outsourcing to TrueCare RCM means every application moves forward on an expedited, parallel-tracked schedule — minimizing the unbillable gap between a physician’s start date and revenue-generating status.
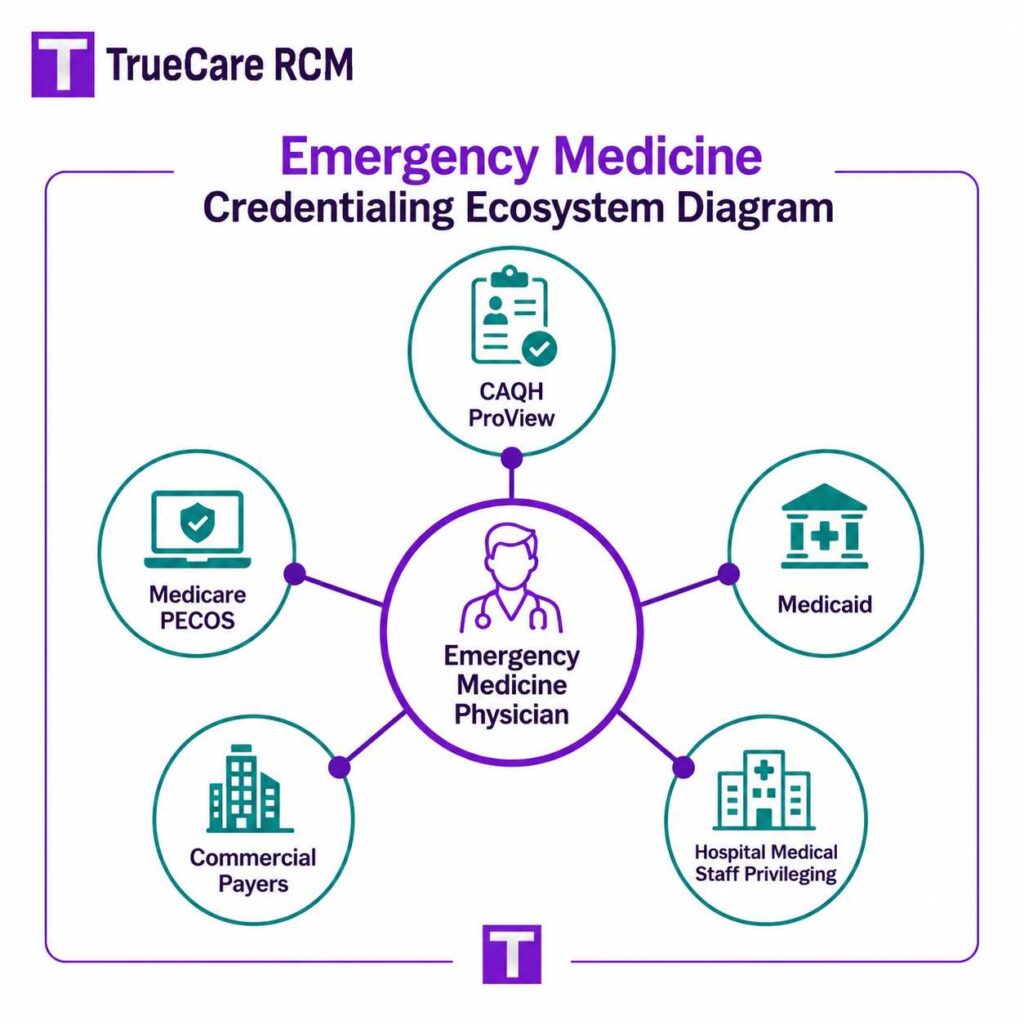
Why Emergency Medicine Credentialing Matters for Group Revenue
Emergency medicine operates under a structural reality most specialties don’t face: physicians often begin clinical coverage based on hospital privileges before payer credentialing is fully resolved, and staffing turnover is high due to locum tenens and rotating coverage models. Getting credentialing wrong — or simply too slow — creates revenue gaps that compound across every new physician a group brings on.
Unlike many specialties, emergency physicians need both standard payer credentialing and hospital medical staff privileging — two separate processes that must both clear before a physician’s care is fully billable in-network. Tracking both simultaneously is essential to avoiding revenue gaps.
Emergency medicine groups frequently rely on locum tenens and rotating physicians, meaning credentialing has to move quickly and repeatedly. Maintaining clean, reusable credentialing files for physicians who work multiple assignments dramatically speeds up each new engagement.
Emergency medicine taxonomy must be applied consistently across NPI, PECOS, CAQH, and every payer application. Incorrect taxonomy assignment leads to payer directory errors and claim denials.
More than 1,400 commercial insurers pull credentials directly from CAQH ProView. A complete, current profile accelerates every commercial application — particularly valuable for emergency physicians who need to onboard with new payers quickly as assignments change.
Hospital privileging runs through the facility’s own medical staff committee, with review cycles that can take 60–120 days and operate independently of payer credentialing timelines. Groups that don’t plan for both tracks in parallel routinely see new physicians sidelined or billing incorrectly.
New emergency medicine groups and newly hired physicians face the longest exposure to credentialing delays since every payer relationship and hospital privilege must be built from zero. Starting both tracks immediately — well before a physician’s first scheduled shift — is the most effective way to minimize unbillable time.
Emergency Medicine Credentialing Documentation Checklist
Before a single application leaves our office, every document needs to be in place. Here’s the full checklist we work through for every emergency medicine physician we credential:
Core Credentials
- MD or DO degree certificate
- Residency completion certificate (ACGME-accredited emergency medicine program)
- Board certification — American Board of Emergency Medicine (ABEM)
- Advanced certifications (ACLS, ATLS, PALS) as required by hospital or payer
Licensing & Registrations
- Current state medical license (in every state where you practice)
- DEA registration certificate
- NPI — both individual (Type 1) and group (Type 2) if applicable
- EIN for group billing
Insurance & Compliance
- Malpractice insurance certificate ($1M/$3M minimum coverage typical)
- Tail coverage documentation if transitioning from a previous assignment
- OIG exclusion check clearance
- NPDB query
Hospital Privileging Documentation
- Hospital-specific medical staff application
- Proof of clinical competency and procedural logs, if required
- Peer references
- Health and immunization records as required by facility policy

Emergency Medicine Credentialing Glossary — Key Terms Explained
| Term | Definition |
| CAQH ProView | Universal credentialing database used by 1,400+ insurers. Requires re-attestation every 120 days. |
| PECOS | CMS Medicare enrollment system. Emergency physicians enroll individually and as part of any group. |
| Hospital Medical Staff Privileging | A separate, hospital-specific credentialing process granting a physician authorization to practice within that facility’s emergency department. |
| ABEM | American Board of Emergency Medicine — the certifying body for emergency physicians. |
| Locum Tenens | Temporary physician staffing arrangements common in emergency medicine, requiring frequent, repeated credentialing across multiple facilities or payer networks. |
| NPI Type 1 / Type 2 | Type 1 is the individual provider identifier; Type 2 is the group/organization identifier. Both required for group billing. |
| Taxonomy Code (Emergency Medicine) | NUCC code identifying a provider’s specialty as emergency medicine, required across PECOS, CAQH, and all payer applications. |
| Reassignment (PECOS) | Process by which an individual provider reassigns Medicare payment rights to a group, filed via CMS-855R. |
| Recredentialing / Revalidation | Re-verification of provider credentials, typically every 2–3 years for commercial payers and every 5 years for Medicare. |
| NPDB | National Practitioner Data Bank — a federal database checked during credentialing for malpractice and licensure history. |
Get Started with Emergency Medicine Credentialing Today
Avoid enrollment delays, protect your revenue, and get your emergency physicians billing in-network faster with TrueCare RCM. Our dedicated credentialing team manages every step — from CAQH setup to hospital privileging coordination — so your group can focus on patient care while we handle the paperwork.
Contact us today for a free credentialing consultation.