Summary:
Provider credentialing is the mandatory process that verifies your qualifications with insurance payers before you can bill for services. For new medical practices, it typically takes 90-120 days and requires complete documentation including licenses, certifications, malpractice insurance, and a CAQH profile. Starting early—ideally 4-6 months before opening—prevents cash flow disruptions and ensures you’re ready to see insured patients from day one.
Table of Contents
- What Provider Credentialing Really Means
- Why You Can’t Skip This Step
- When to Start the Credentialing Process
- The Complete Documentation Checklist
- Understanding CAQH: Your Credentialing Foundation
- Credentialing vs. Enrollment: Know the Difference
- Medicare and Medicaid Credentialing Essentials
- Individual vs. Group Credentialing Strategies
- Common Delays and How to Avoid Them
- The Cash Flow Reality for New Practices
- Should You Outsource Credentialing?
- Frequently Asked Questions
What Provider Credentialing Really Means (And Why It Feels Like a Background Check)
Look, I’ll be straight with you: provider credentialing is essentially insurance companies doing their homework on you. They want to verify you’re legit, qualified, and not a risk before they start cutting you checks for patient care.
Here’s what actually happens: Insurance payers—think Blue Cross Blue Shield, Aetna, UnitedHealthcare, and government programs like Medicare and Medicaid—review your credentials to confirm you meet their participation standards. They’re checking your medical education, board certifications, state licenses, work history, malpractice insurance, and even your disciplinary record.
For new medical practices, this isn’t just a formality. It’s the gateway to revenue. Without completed credentialing, you can’t submit claims to insurance companies. You can see patients, sure—but you’ll need to collect payment directly from them, which severely limits your patient base and income potential.
The process involves submitting applications to each payer you want to work with, maintaining a CAQH profile (more on that shortly), and then waiting. Sometimes for months. It’s bureaucratic, it’s tedious, and yes, it’s absolutely mandatory if you want to participate in insurance networks.

Why Provider Credentialing Is Required Before Billing Insurance (No Exceptions)
You might be wondering: can’t I just start seeing patients and figure this out later? The answer is a hard no—at least not if you want insurance to pay you.
Here’s the thing: insurance credentialing establishes you as an approved, in-network provider. Without it, claims submitted under your NPI (National Provider Identifier) will be rejected faster than you can say “prior authorization.” Payers maintain strict provider networks, and if you’re not in their system, your claims don’t get processed.
But there’s more to it than just getting paid. Credentialing also:
- Protects patients by ensuring they have access to qualified, vetted healthcare providers
- Reduces fraud in the healthcare system by verifying provider identities and credentials
- Establishes your effective date with each payer, which determines when your services become billable
- Enables you to accept insurance that most patients rely on for coverage
- Affects your practice’s reputation since patients trust credentialed providers more
The relationship between credentialing and medical billing is inseparable. Your billing team can’t submit clean claims without proper credentialing, and delays in credentialing mean delays in revenue. For new practices operating on tight budgets, this can be catastrophic.
When Should a New Medical Practice Start the Credentialing Process? (Spoiler: Yesterday)
Timing is everything with provider credentialing. Start too late, and you’ll open your doors with no way to bill insurance for months. That’s a recipe for financial disaster.
The ideal timeline: Begin your credentialing process 4-6 months before you plan to see your first patient. Yes, months. I know it sounds excessive, but here’s why:
Typical credentialing timelines by payer:
| Payer Type | Average Timeline | Notes |
| Medicare (PECOS) | 60-90 days | Can be faster with complete applications |
| Medicaid | 60-120 days | Varies significantly by state |
| Commercial Insurance (BCBS, Aetna, etc.) | 90-120 days | Some payers take up to 180 days |
| Managed Care Plans | 60-90 days | Often faster than traditional insurance |
These timelines assume everything goes smoothly—no missing documents, no verification delays, no payer backlogs. In reality, you should plan for the upper end of these ranges.
Critical milestones for new practices:
- 6 months before opening: Obtain your NPI, set up your CAQH profile, gather all required documents
- 4-5 months before opening: Submit applications to Medicare, Medicaid, and top commercial payers
- 3 months before opening: Follow up on all applications, respond to any requests for additional information
- 2 months before opening: Confirm effective dates, ensure all approvals are in place
- 1 month before opening: Verify billing systems are configured with correct payer IDs and provider numbers
For multi-provider practices, stagger your credentialing to ensure at least one provider is approved before opening. This gives you some revenue stream while waiting on others.
The Complete Documentation Checklist (Don’t Skip a Single Item)
Missing even one document can add weeks to your credentialing timeline. Here’s exactly what you need, organized by category:
Professional Credentials
- Medical degree (MD, DO) or professional degree (DPM, DC, etc.)
- Board certification documents (if applicable)
- State medical license (current and valid)
- DEA certificate (if prescribing controlled substances)
- State controlled substance license (varies by state)
- NPI (National Provider Identifier)
Practice Information
- Tax ID (EIN) for your practice
- Practice location address and contact information
- Business license
- Office hours and patient capacity
- Hospital affiliations (if any)
Insurance and Liability
- Professional liability insurance (malpractice) – typically $1M/$3M minimum
- Certificate of insurance with current coverage dates
- General liability insurance for your practice location
Work History and References
- Complete work history for the past 10 years (some payers require 5-7 years)
- Three professional references (usually physician colleagues)
- Hospital privileges documentation (if applicable)
- Academic appointments (if applicable)
Background Verification
- NPDB (National Practitioner Data Bank) self-query report
- State medical board verification
- Medicare opt-out status (if applicable—most new practices do NOT opt out)
- Sanctions screening clearance (OIG, SAM, etc.)
CAQH-Specific Documents
- CV or résumé in standard format
- Professional headshot (yes, really)
- Practice liability insurance face sheet
- W-9 form for tax reporting
Pro tip: Create digital copies of everything and organize them in clearly labeled folders. You’ll submit the same documents multiple times to different payers, and having them readily accessible saves enormous time.
What Is CAQH and Is It Mandatory for Credentialing? (Yes, and Here’s Why)
CAQH ProView is the central hub that makes provider credentialing possible without losing your mind. Think of it as the common application for healthcare provider credentialing.
What CAQH actually does: The Council for Affordable Quality Healthcare (CAQH) maintains a universal database where you input all your credentialing information once. Participating insurance companies then access your CAQH profile instead of making you fill out individual applications for each payer.
Over 1,400 health plans use CAQH ProView, including virtually every major commercial insurance company. Medicare and some state Medicaid programs don’t use CAQH, but nearly everyone else does.
Is it mandatory? Technically, CAQH itself isn’t legally required—but practically speaking, yes. Without a complete, attested CAQH profile, you cannot credential with the vast majority of commercial payers. It’s free for providers, and refusing to use it would be like refusing to use email for professional communication.
Setting Up Your CAQH Profile: The Right Way
- Register at caqh.org using your NPI
- Complete every single section – incomplete profiles delay credentialing
- Upload all supporting documents in the formats specified
- Attest your profile (this step is critical and often overlooked)
- Re-attest every 120 days to keep your profile active
Common CAQH mistakes that kill credentialing timelines:
- Leaving sections blank instead of marking them “N/A”
- Uploading expired insurance certificates
- Forgetting to attest after making updates
- Using incorrect date formats
- Failing to update when credentials change
Your CAQH profile is your credentialing foundation. Get it perfect from the start, and you’ll save yourself countless hours of back-and-forth with payers.

Provider Credentialing vs. Enrollment: They’re Not the Same Thing
People use these terms interchangeably, and honestly, it’s confusing as hell. But there’s a real difference that matters for your practice workflow.
Provider credentialing is the verification process. It’s when payers review your qualifications, background, and documentation to determine if you meet their participation requirements. Think of it as the vetting stage.
Provider enrollment is what happens after you’re credentialed. It’s the administrative process of actually adding you to the payer’s network, assigning you provider numbers, and establishing your effective date for claims submission. This is the “you’re in” stage.
Here’s how it typically flows:
- You submit credentialing applications
- Payer verifies your credentials (credentialing)
- Once approved, payer processes enrollment paperwork
- You receive provider numbers and effective dates
- You can now submit claims for reimbursement
For Medicare, the process is called “enrollment” but includes credentialing steps—they verify everything through PECOS (Provider Enrollment, Chain and Ownership System). Medicaid varies by state, with some using the term “enrollment” and others using “credentialing.”
Why this distinction matters: You might be “credentialed” but not yet “enrolled,” which means you still can’t bill. Always confirm your enrollment is complete AND you have your effective date before submitting claims.

Medicare and Medicaid Credentialing for New Practices (The Government Programs)
Government payer credentialing comes with its own special flavor of bureaucracy. Let’s break down what you need to know.
Medicare Credentialing via PECOS
Medicare enrollment happens through PECOS, and it’s non-negotiable if you want to see Medicare patients (which, let’s be real, most practices do).
Key requirements:
- Completed CMS-855 application (855I for individuals, 855B for groups)
- Valid state medical license
- Board certification (if applicable)
- Practice location with a physical address (no P.O. boxes)
- Compliance with all Medicare regulations
Timeline: 60-90 days typically, though incomplete applications get rejected and restart the clock.
Critical detail: Medicare has a “look-back” period for revalidation. Even as a new practice, you’ll need to revalidate your enrollment every 5 years, and Medicare will notify you 6 months before your deadline.
Medicaid Enrollment by State
Here’s where things get complicated: Medicaid is administered at the state level, so requirements vary wildly. A practice credentialing in California faces completely different requirements than one in Texas or New York.
State-specific variations:
| State | Typical Timeline | Special Requirements |
| California | 90-120 days | Additional state background checks |
| Texas | 60-90 days | Texas-specific provider agreements |
| Florida | 90-120 days | AHCA registration required |
| New York | 90-150 days | eMedNY enrollment mandatory |
| Illinois | 60-90 days | HFS provider enrollment |
If you’re credentialing in multiple states—common for telehealth providers or multi-location practices—each state requires separate Medicaid enrollment.
Pro tip: Some states have faster processing for certain specialties (pediatrics, behavioral health) due to provider shortages. Check your state’s Medicaid website for specialty-specific programs.

Individual vs. Group Credentialing: Which Strategy Works for Your Practice?
The structure of your practice determines your credentialing approach, and choosing the wrong one complicates everything.
Individual credentialing means each provider in your practice credentials separately under their own NPI. They’re treated as independent practitioners, even if they work under the same practice umbrella.
Group credentialing means your practice credentials as an organization, and individual providers are added as members of that group under the group NPI.
When to Use Individual Credentialing
- Solo practitioners
- Independent contractors in a shared space
- Practices where providers have different specialties
- Situations where providers might leave and establish their own practices
When to Use Group Credentialing
- Multi-provider practices with shared ownership
- Practices where providers are W-2 employees
- When you want centralized billing and administration
- For consistency in payer contracts and reimbursement rates
The hybrid approach: Many practices use both. The group credentials for organizational purposes, and individual providers also maintain their own credentialing for flexibility. This provides backup options if someone leaves or if certain payers require individual participation.
Cash flow consideration: Group credentialing can sometimes be faster because you’re submitting one comprehensive application instead of multiple individual ones. However, if your group application gets delayed, all providers are stuck waiting.
For new practices with multiple providers, I generally recommend starting individual credentialing processes first, then pursuing group credentialing once you’re established. This hedges your risk.

What Causes Credentialing Delays for New Practices (And How to Avoid Them)
Let me tell you the most frustrating thing about credentialing: preventable delays that add months to your timeline. Here are the top culprits:
- Incomplete Applications
The problem: Missing even a single signature or document triggers a rejection. The fix: Use a credentialing checklist and have someone else review your applications before submission.
- CAQH Profile Not Attested
The problem: You can have a perfect CAQH profile, but if you don’t click “attest,” payers can’t access it. The fix: Attest immediately after completing your profile, and set calendar reminders for re-attestation every 120 days.
- Expired Documents
The problem: Your malpractice insurance or state license expires during the credentialing process. The fix: Ensure all documents are valid for at least 6 months beyond your application date.
- Unresponsive References
The problem: Payers can’t reach your professional references, stalling verification. The fix: Give references a heads-up, confirm their contact information, and choose people who respond quickly.
- Hospital Privileges Verification Delays
The problem: Hospitals take forever to verify your privileges (if applicable). The fix: Request verification letters from hospitals at the start of credentialing, not when payers ask.
- Payer Backlogs
The problem: Insurance companies are overwhelmed and processing slowly. The fix: Submit applications during off-peak times (avoid January and July when many new providers start), and follow up weekly.
- Address Mismatches
The problem: Your practice address on your license doesn’t match your CAQH profile or payer application. The fix: Ensure complete consistency across all documents—same format, same suite numbers, everything.
- Missing State-Specific Requirements
The problem: Some states require additional credentialing steps you didn’t know about. The fix: Research state-specific requirements early, especially for Medicaid.
Real talk: The single biggest cause of delays is simply not following up. Payers won’t chase you. Set a schedule to check on every application weekly, and don’t be afraid to call and email.
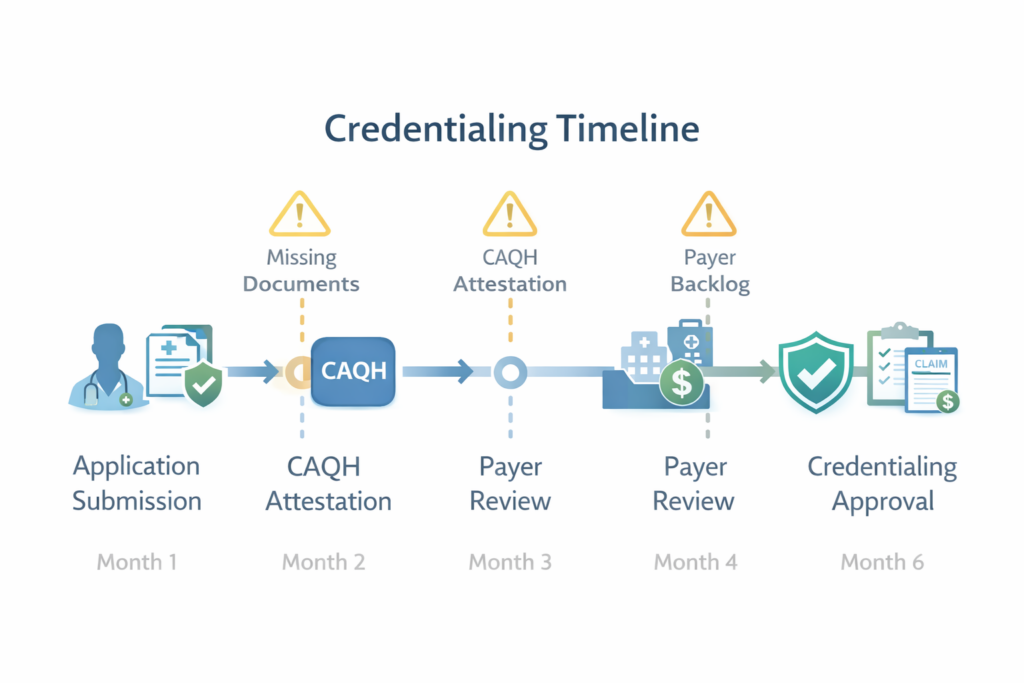
Insert image of credentialing timeline with common delay points marked here

How Credentialing Affects Cash Flow for Medical Practice Startups (The Brutal Truth)
Let’s talk money, because this is where credentialing hits hardest for new practices.
You’ve invested everything into opening your practice—lease deposits, equipment, staff salaries, insurance, supplies. You’re hemorrhaging cash before you see a single patient. And then credentialing adds 3-4 months where you can see patients but can’t bill their insurance.
The cash flow gap looks like this:
Months 1-4: Credentialing in process
- Expenses: Running at 100%
- Revenue: $0 from insurance (maybe some self-pay)
- Burn rate: Maximum
Months 5-6: Credentialing complete, seeing patients
- Expenses: 100%
- Revenue: Still $0 (claims processing takes 30-45 days)
- Burn rate: Still very high
Months 7-8: First insurance payments arrive
- Expenses: 100%
- Revenue: 30-50% of expected (ramp-up period)
- Burn rate: Decreasing
This means new practices need 6-8 months of operating capital minimum. Many fail because they underestimate this timeline.
Strategies to Manage Cash Flow During Credentialing
- Start credentialing before you’re ready to see patients. Seriously. Begin 6 months out.
- Consider accepting self-pay patients initially with discounted rates to generate some revenue.
- Negotiate delayed lease or equipment payments for the first few months if possible.
- Line up a business line of credit before you need it—banks are more willing to lend before you’re desperate.
- Credential strategically. Focus first on payers who cover most patients in your area and process faster.
- Track every application obsessively so you know exactly when revenue will start flowing.
- Request retroactive billing when possible (more on this shortly).
The practices that survive credentialing delays are the ones that plan for the worst-case scenario financially.
Should New Practices Outsource Provider Credentialing? (Here’s My Take)
You can absolutely handle credentialing yourself. You can also perform your own dental work, but that doesn’t mean you should.
The DIY approach works if:
- You have significant administrative time available
- You’re credentialing as a single provider
- You’re only applying to 3-5 payers
- You’re extremely detail-oriented and organized
- You have experience with healthcare administration
Outsourcing makes sense if:
- You’re opening a multi-provider practice
- You want to focus on clinical work, not paperwork
- You’re credentialing with 10+ payers
- You need to meet tight opening deadlines
- You can’t afford delays that cost thousands in lost revenue
What Credentialing Services Actually Do
Professional credentialing services like TrueCare RCM handle the entire process:
- Application management: Complete and submit all payer applications
- CAQH profile setup and maintenance: Ensure your profile stays current and attested
- Document verification: Gather and organize all required documentation
- Follow-up and tracking: Regular status checks with every payer
- Delay resolution: Direct payer communication to resolve issues quickly
- Recredentialing: Manage ongoing compliance and revalidation
The cost: Credentialing services typically charge per provider per payer, ranging from $100-300 per application, or offer packages for comprehensive credentialing.
The ROI calculation: If outsourcing saves you even 2-4 weeks per payer, and each week of delay costs you $5,000-10,000 in lost revenue, the math is simple. A $2,000 investment in credentialing services easily pays for itself many times over.
My honest recommendation: For new practices, outsource it. Your time is better spent on patient care, marketing, and practice operations. Credentialing requires specialized knowledge of payer requirements, and mistakes are expensive. Services like TrueCare RCM have established relationships with payers and know exactly how to navigate their systems efficiently.
Ready to Start Your Medical Practice the Right Way?
Provider credentialing isn’t glamorous, but it’s the foundation of your practice’s financial viability. Start early, stay organized, and don’t underestimate the complexity.
For new medical practices in California, Texas, Florida, New York, or anywhere across the country, TrueCare RCM provides comprehensive credentialing services that eliminate the guesswork and accelerate your time to revenue. We handle everything from CAQH profile setup to Medicare enrollment to commercial payer credentialing—for every specialty from family practice to behavioral health to ambulatory surgical centers.
Get your credentialing started right:
- Schedule a consultation: Contact TrueCare RCM at (323) 538-6467
- Email us: info@truecarercm.com
- Visit: https://truecarercm.com/
- Location: 8674 Falmouth Ave #306, Playa Del Rey, CA 90293
We’ve credentialed hundreds of providers across all specialties and know exactly how to navigate payer requirements efficiently. Let us handle the paperwork so you can focus on what matters—providing excellent patient care.
Don’t let credentialing delays cost you months of revenue. Start the process today.


