Nurse practitioner credentialing is the formal process of verifying your qualifications so insurance companies approve you to bill for patient services. It typically takes 60–150 business days, requires documents like your NPI, Malpractice Coverage, Board Certification, and DEA Certificate, and involves payers including Medicare, Medicaid, and commercial insurers. Outsourcing to a professional credentialing service like TrueCare RCM dramatically reduces errors, delays, and revenue loss — especially for new practices, multi-state NPs, and telehealth providers.
Learn more about how our Provider Enrollment & Credentialing Services streamline the entire process and reduce delays.
Table of Contents
- What Is Nurse Practitioner Credentialing?
- Why NP Credentialing Is Critical in 2026
- Step-by-Step NP Credentialing Process
- Required Documents for NP Credentialing
- How Long Does NP Credentialing Take?
- How Much Do Credentialing Services Cost?
- Medicare Enrollment: The PECOS Pathway
- Medicaid Enrollment for Nurse Practitioners
- What Is CAQH — And Why It Can Make or Break You
- Specialty-Specific Credentialing Considerations
- State-Specific NP Credentialing Requirements
- Credentialing for Telehealth Nurse Practitioners
- Common NP Credentialing Mistakes & How to Avoid Them
- Recredentialing & Ongoing Compliance
- Does Credentialing Affect Billing and Reimbursement?
- Benefits of Outsourcing NP Credentialing Services
- Frequently Asked Questions (FAQs)
1. What Is Nurse Practitioner Credentialing?
Let’s be real — credentialing is one of the most unglamorous parts of launching or running an NP practice. It’s the administrative mountain you climb before you can get paid a single dollar from insurance. But ignore it, and that mountain turns into a cliff.
Nurse practitioner credentialing is the formal process of verifying a provider’s qualifications, licenses, certifications, training, and professional history so that insurance companies and government payers approve them for reimbursement. In short, it confirms you meet payer network participation standards before you can submit — and actually get paid for — claims.
Credentialing vs. Provider Enrollment: What’s the Difference?
These two terms are often used interchangeably, but they mean different things:
- Credentialing = Verification of your education, training, licensure, work history, and professional background.
- Provider Enrollment = Registering with Medicare, Medicaid, and commercial payers to obtain billing privileges.
Both are required before reimbursement can begin. Think of credentialing as your professional background check and provider enrollment as actually getting your name on the approved billing list. One confirms who you are; the other unlocks the revenue.
2. Why NP Credentialing Is More Critical Than Ever in 2026
Healthcare regulations, payer standards, and the explosion of telehealth have made credentialing more complex — and more consequential — than at any point in recent history. Here’s what’s driving the stakes higher:
| Challenge in 2026 | Impact on NPs |
| Tightening commercial payer standards | More documentation, stricter compliance checks |
| CMS enrollment updates (Medicare/Medicaid) | Accuracy is non-negotiable; errors trigger audits |
| Telehealth & multi-state practice expansion | Simultaneous multi-state licensing & enrollment required |
| Revenue cycle pressure | Delayed credentialing = denied claims, lost revenue |
The bottom line: credentialing is directly tied to your revenue cycle performance. Without it, claims cannot be paid, networks cannot be accessed, and compliance risks multiply. Getting it right — and getting it done on time — is foundational to a sustainable practice in 2026.
3. Step-by-Step Nurse Practitioner Credentialing Process
Understanding each phase of the process is the single best thing you can do to prevent delays. Here’s exactly how NP insurance credentialing works from start to finish:
Step 1: Obtain Your NPI & Confirm Active Licensure
- National Provider Identifier (NPI) — issued via NPPES; your permanent professional ID
- Active RN and NP license(s) for each state you practice in
- Board certification (e.g., FNP-C, PMHNP-BC, AGPCNP-BC)
- DEA registration if prescribing controlled substances
Step 2: Secure Malpractice Insurance
Most payers require proof of active professional liability coverage with minimum liability limits. Make sure your effective dates are current and that your policy details exactly match what you’ll enter on credentialing applications — even a small mismatch can trigger delays.
Step 3: Set Up Your CAQH ProView Profile
CAQH is the centralized credentialing data hub used by most commercial payers. Complete your profile with:
- License copies and board certifications
- DEA certificate
- Malpractice insurance certificate
- Work history (minimum 5 years)
- Education and training history
- Professional references
Critical: Your CAQH profile must be marked as ‘Authorized to Release’ before payers can access it. And you must reattest every 120 business days — or your profile expires and the clock resets.
Step 4: Medicare Enrollment via PECOS
Enrollment is completed through CMS’s Provider Enrollment, Chain, and Ownership System (PECOS) using the CMS-855I form. You’ll also need to complete an Electronic Funds Transfer (EFT) setup for direct deposit of Medicare payments. Average processing time: 60–90 business days.
Most common Medicare delay triggers: incomplete applications, mismatched NPI/TIN data, incorrect taxonomy codes.
Step 5: Medicaid Provider Enrollment
Each state Medicaid program has its own portal, documentation requirements, and approval timeline. Timelines range from 45 to 120+ business days depending on the state. Some states require additional background screening.
Step 6: Commercial Insurance Panel Enrollment
This includes major carriers like Blue Cross Blue Shield, Aetna, UnitedHealthcare, Cigna, Humana, and regional managed care plans. Average approval time: 60–120 business days. Note: some panels may be closed in saturated markets, so check network status before applying.
Step 7: Primary Source Verification & Final Approval
Payers independently verify your license status, board certification, education credentials, malpractice claims history, and any sanctions or exclusions. Once all checks clear, you’ll receive final approval and your contract activation date — which becomes your effective billing date.
For dedicated support throughout this process — from CAQH setup to payer follow-up — explore our Provider Enrollment & Credentialing Services.
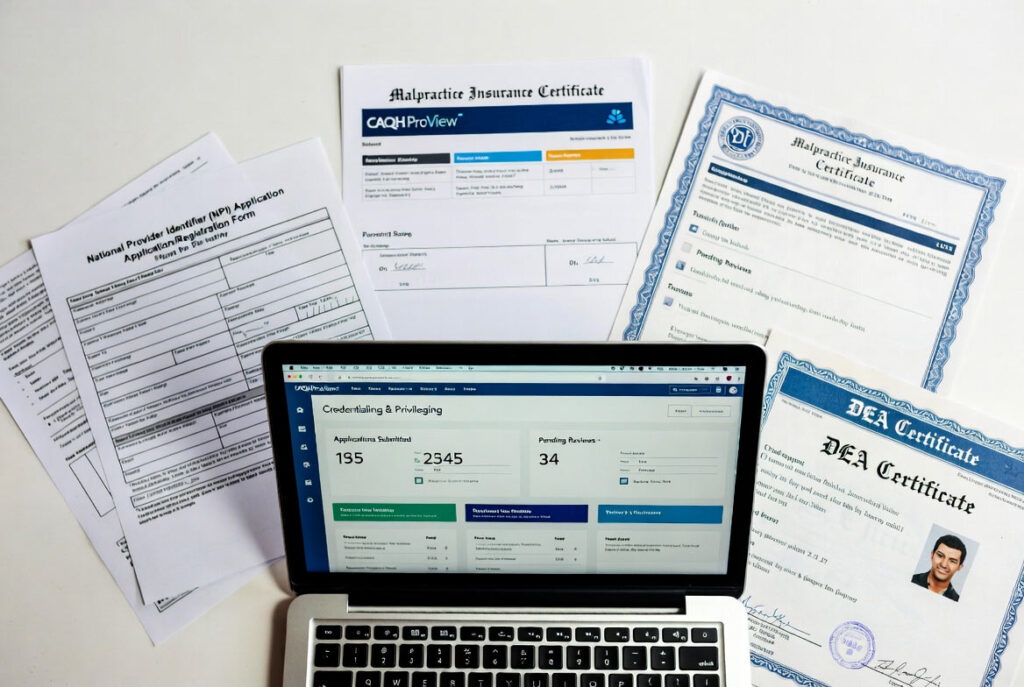
4. Required Documents for NP Credentialing
Getting your documentation checklist right the first time prevents months of back-and-forth. Here’s what you’ll almost always need:
- Active NP license (and RN license where required)
- National Provider Identifier (NPI) — individual and group NPI if applicable
- Board certification credentials (AANP, ANCC, etc.)
- DEA Certificate (if prescribing controlled substances)
- Professional malpractice insurance certificate with coverage limits and effective dates
- CV or work history covering the last 5–10 years
- Collaborative practice agreement (required in some states)
- Government-issued photo ID
- Tax Identification Number (TIN) / EIN for your practice
- Proof of clinical training and education
- CAQH ProView login with completed, authorized attestation
- Hospital privileges documentation (if applicable)
Missing even one of these can throw your entire application into a holding pattern. Credentialing coordinators will tell you: incomplete documentation is the single biggest cause of delays.
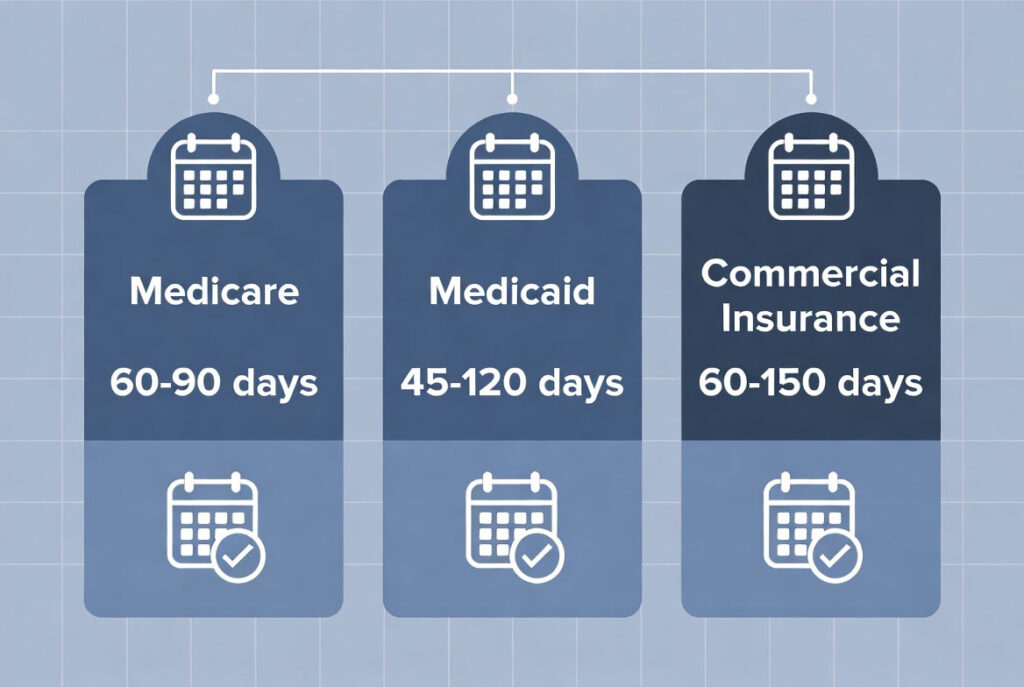
5. How Long Does Nurse Practitioner Credentialing Take in 2026?
Everyone wants a magic number. Here’s a realistic breakdown by payer type — plus the factors that can push these timelines in either direction:
| Payer Type | Average Timeline | Notes |
| Medicare (PECOS) | 60–90 business days | Required for all federal billing |
| Medicaid | 45–120 business days | Varies significantly by state |
| Commercial Insurers | 60–150 business days | e.g., Aetna, BlueCross, UHC |
| CAQH Setup | 1–2 weeks | Must be completed first |
| Hospital Privileges | 60–180 business days | Depends on facility credentialing committee |
Factors That Cause Delays
- Incomplete or inaccurate CAQH profiles
- Expired documents submitted with applications
- Incorrect provider taxonomy codes
- No proactive follow-up with payer credentialing departments
- Closed insurance panels in your market
How to Speed Things Up
- Prepare and verify all documents before submitting any application
- Double-check NPI and TIN accuracy across every form
- Maintain CAQH accuracy and keep attestation current
- Follow up weekly with payers — silence is not approval
- Work with experienced NP credentialing specialists who know payer timelines
Bottom line: plan for 90–120 business days on average, start 3–6 months before your target launch date, and build in buffer. Some payers move fast. Others still operate at the speed of fax machines. (Yes, some still use them.)
6. How Much Do Credentialing Services for Nurse Practitioners Cost?
Let’s talk money. Here’s an honest breakdown of NP credentialing service costs in 2026:
| Service | Typical Cost Range |
| Per-payer applications (à la carte) | $150–$400 per payer |
| Medicare PECOS Enrollment | $250–$500 |
| Medicaid Enrollment | $200–$500 |
| Full-Service Credentialing Package | $1,200–$3,500 per provider |
| Ongoing Recredentialing / Maintenance | $500–$1,500/year |
| CAQH Setup & Attestation | Often included in full-service packages |
The Real Cost of Delays
A 90-day credentialing delay can cost an NP practice anywhere from $20,000 to $80,000 or more in lost revenue — depending on your specialty, patient volume, and payer mix. Suddenly, a full-service credentialing package at $1,500–$3,500 looks like a very smart investment.
Here’s the thing about DIY credentialing: the money you save upfront is almost always outweighed by the revenue you lose while you’re stuck in payer limbo, trying to figure out why your CAQH won’t authorize or why Medicare keeps asking for the same document twice. Outsourcing credentialing often pays for itself within your first week of billing.
See how our Provider Enrollment & Credentialing Services can reduce delays and deliver ROI by accelerating approvals.

7. Medicare Enrollment for Nurse Practitioners: The PECOS Pathway
How Do NPs Get Credentialed with Medicare?
Getting credentialed with Medicare requires enrolling through PECOS — the Provider Enrollment, Chain, and Ownership System. Here’s the step-by-step:
- Register or log in to the CMS Enterprise Identity Management (EIDM) system.
- Access PECOS and select ‘Start a New Enrollment.’
- Select your enrollment type: Individual Practitioner.
- Complete all sections: personal info, practice location, NP specialty, and billing information.
- Upload supporting documents as prompted by the portal.
- Complete EFT setup for direct payment to your practice bank account.
- Submit and track your application via the CMS Application Status tool.
Medicare enrollment for NPs typically takes 60–90 business days. The most common delay triggers: mismatched NPI and tax ID data, incorrect NP taxonomy codes, and incomplete application sections. Getting these details exactly right the first time saves weeks.
8. Medicaid Enrollment for Nurse Practitioners
Medicaid is state-run — which means the process, timeline, and requirements are different in every state. California has Medi-Cal. Georgia has Georgia Medicaid. Texas has Texas Medicaid. Each has its own portal, its own quirks, and its own timeline.
Generally, you’ll need to:
- Register on your state’s Medicaid provider enrollment portal
- Submit NPI, TIN, and license information
- Upload malpractice insurance and collaborative agreements where required
- Complete a background check (state-dependent)
- Wait for verification and assignment of a Medicaid Provider ID
In states like North Carolina, Virginia, and Minnesota, Medicaid enrollment can take 3–5 months or more. Starting early and submitting error-free applications isn’t just good advice — it’s the only strategy that works.
9. What Is CAQH — And Why It Can Make or Break Your Credentialing
CAQH ProView is essentially the LinkedIn profile of healthcare credentialing — except far more consequential, and much less fun to fill out.
CAQH (Council for Affordable Quality Healthcare) is a centralized database where you upload your professional credentials once, and participating health plans can access your information without requiring you to resubmit the same documents 20 times over.
Why CAQH Matters for NPs:
- Most major commercial payers require a completed, authorized CAQH profile before processing your application
- It eliminates redundant paperwork across participating payers
- You must reattest every 120 business days — or your profile expires and credentialing stalls
- Your profile must be marked ‘Authorized to Release’ for any payer to access it
- Inaccurate or outdated CAQH data propagates errors across every payer application you submit
Think of CAQH as the foundation your entire credentialing house is built on. If the foundation is cracked — expired, unauthorized, or inaccurate — the whole structure is compromised. Setting it up correctly from the start, and maintaining it religiously, is one of the highest-leverage actions you can take.
10. Specialty-Specific NP Credentialing Considerations
Your specialty shapes your credentialing experience in ways that most generic guides don’t acknowledge. Different NP specialties face distinct documentation requirements, payer scrutiny levels, and enrollment hurdles. Here’s a practical breakdown:
| Specialty | Key Credentialing Considerations |
| Family Practice NP | Highest payer volume; broad Medicare/Medicaid exposure |
| Psychiatric / Behavioral Health NP | Managed care network limitations; PMHNP-BC required |
| Dermatology NP | Procedural experience documentation; pre-auth credentialing |
| Orthopedic NP | Surgical privileges scrutiny; hospital facility credentialing |
| Anesthesiology NP | Hospital credentialing alongside payer enrollment |
| Home Health NP | CMS face-to-face documentation; dual Medicare/managed care enrollment |
| Physical / Occupational Therapy NP | May require supervising physician enrollment linkage |
The takeaway: specialty-specific credentialing nuances are exactly where DIY applications most often go wrong. An experienced NP credentialing company will know the payer-specific documentation requirements for your specialty before you even submit.
For tailored revenue cycle support including credentialing and billing, see our Medical Billing & Coding Services and Internal Medicine Billing & Credentialing Services pages.
11. State-Specific NP Credentialing Requirements
State laws around nurse practitioner practice, collaborative agreements, and Medicaid enrollment vary enormously. Here’s a snapshot of the 12 states TrueCare RCM proudly serves, with key state-specific considerations:
- California (CA) — Full practice authority in many settings; Medi-Cal enrollment required for Medicaid billing; some of the most complex commercial payer landscapes in the country
- Texas (TX) — Collaborative agreement required; Texas Medicaid has detailed eligibility requirements and a state-specific portal
- Florida (FL) — Collaborative agreement required; one of the longer Medicaid credentialing timelines; Managed Medical Assistance program adds complexity
- New York (NY) — Full practice authority (as of 2023); Empire Plan credentialing is separate from standard commercial enrollment
- Georgia (GA) — Collaborative agreement required; Georgia Medicaid portal can be slow; allow extra lead time
- North Carolina (NC) — Collaborative agreement required; Medicaid managed care transition (NC Medicaid Managed Care) affects enrollment significantly
- Arizona (AZ) — Full practice authority; AHCCCS Medicaid enrollment required; telehealth NPs face multi-state complexity
- Illinois (IL) — Full practice authority; Illinois Medicaid has specific portal requirements and enrollment timelines
- Minnesota (MN) — Full practice authority; Minnesota Health Care Programs (MHCP) enrollment required for Medicaid
- Michigan (MI) — Collaborative agreement required; Michigan Medicaid portal has unique steps and can require additional documentation
- Maryland (MD) — Full practice authority; Maryland Medicaid enrollment via eMedicaid system
- Virginia (VA) — Full practice authority (2023); Virginia Medicaid credentialing via the Inovalon provider portal
Multi-state credentialing requires careful planning to avoid overlapping compliance issues, mismatched documentation, and missed deadlines. If you’re practicing across state lines — especially via telehealth — this is where professional credentialing support pays the biggest dividends.
TrueCare RCM provides credentialing and enrollment support in all these states — learn more on our Provider Enrollment & Credentialing Services
page.

12. Credentialing for Telehealth Nurse Practitioners
Telehealth has exploded — but the credentialing requirements haven’t gotten simpler. If anything, practicing across state lines adds a layer of complexity that catches a lot of NPs off guard.
Multi-State Licensing
Telehealth NPs must hold a valid, active license in every state where their patients are physically located at the time of the visit. The Nurse Licensure Compact (NLC) allows multi-state practice under a single license in participating states — but not all states are NLC members, and those that aren’t require separate state licensure.
Telehealth Payer Enrollment
Many insurers require separate state-specific enrollment for telehealth services. This includes:
- Updated practice address or telehealth service location designation
- State-specific Medicaid telehealth enrollment
- Telehealth modifier documentation for claims
If you’re launching a telehealth NP practice in 2026, build in additional lead time for multi-state credentialing — and consider professional support from a company experienced in cross-state NP enrollment.
13. Common NP Credentialing Mistakes — And How to Avoid Them
We’ve seen it all. Here are the mistakes that cause the vast majority of NP credentialing delays and denials:
- Submitting incomplete or inaccurate credentialing applications to payers
- CAQH profile not authorized for release — or expired attestation
- Malpractice insurance gaps, wrong effective dates, or incorrect policy limits listed
- NPI not correctly linked to your group practice TIN
- Wrong or missing provider taxonomy codes on Medicare/Medicaid applications
- Missing collaborative practice agreements in states that require them
- Applying to closed insurance panels without verifying network status
- Underestimating the credentialing timeline and missing your practice launch target
- No proactive follow-up — assuming silence from payers means progress
- Failing to track application status and deadlines across multiple payers
Avoiding these mistakes can reduce your approval timeline by weeks — sometimes months. And if this list feels overwhelming? That’s a strong signal it’s time to outsource.
14. Recredentialing & Ongoing Compliance
Credentialing isn’t a one-and-done event. It’s an ongoing obligation — and failing to keep up can get you removed from payer networks, trigger claim denials, and create revenue gaps that take months to recover from.
Recredentialing Frequency
- Most payers require full recredentialing every 2–3 years
- CAQH attestation required every 120 days
Ongoing Compliance Checklist
- Maintain active, current licenses in all practicing states
- Keep malpractice insurance active with no coverage gaps
- Renew board certifications on schedule
- Update CAQH immediately when any credential information changes
- Notify payers of practice address changes, new group affiliations, or added specialties
Network termination from missed recredentialing is more common than most NPs realize — and it can happen quietly, with little warning. Build a recurring calendar system for credential expiration dates, or work with a credentialing service that monitors this proactively.
15. Does Credentialing Affect NP Billing and Reimbursement?
Short answer: massively. Long answer: here’s exactly how.
Until you’re fully credentialed and enrolled with a payer, you cannot bill that payer for services — full stop. Claims submitted before your effective participation date will be denied. And many payers won’t allow retroactive billing for services rendered during your pending credentialing period, meaning that revenue is simply gone.
This is why a 90-day credentialing delay isn’t just a paperwork headache — it’s a $20,000–$80,000+ revenue problem, depending on your specialty and patient volume. Every week you’re not credentialed with Medicare, Medicaid, and major commercial plans is money that doesn’t come back.
Credentialing is revenue cycle management. Treat it that way from day one.
16. Benefits of Outsourcing NP Credentialing Services
Managing credentialing internally is manageable if you have the time, the expertise, and the patience for payer follow-up. Most NPs don’t — and shouldn’t have to. Here’s what professional outsourced credentialing delivers:
- Faster payer approvals from experienced specialists who know exactly what each payer needs
- Dedicated, proactive follow-up with insurance networks — no application left sitting
- Dramatically reduced administrative burden on your practice staff
- Improved billing readiness from day one of your effective date
- Compliance accuracy across Medicare, Medicaid, and commercial payer requirements
- Multi-state and multi-specialty credentialing expertise
- Transparent reporting so you always know where every application stands
- Ongoing recredentialing management and CAQH maintenance
Outsourcing allows NPs and practice administrators to focus on patient care — not paperwork. And in a landscape where every week of delay costs real money, having credentialing experts in your corner isn’t a luxury. It’s a smart business decision.
Our outsourced credentialing solutions are part of a full RCM offering. Visit Medical Billing & Coding Services to see how we integrate credentialing into end-to-end revenue management.
17. Frequently Asked Questions About NP Credentialing
Q1: What is nurse practitioner credentialing?
NP credentialing is the formal verification process required before insurance companies authorize reimbursement. Payers verify your licenses, certifications, work history, and professional background before granting billing privileges.
Q2: How long does NP credentialing take?
Typically 60–150 business days, depending on the payer and state. Medicare (PECOS) takes 60–90 business days; Medicaid ranges from 45–120 business days by state; commercial payers average 60–120 business days. Plan for 90–120 business days as a realistic baseline.
Q3: What documents are required for NP credentialing?
Active NP and RN licenses, board certification, DEA certificate (if applicable), malpractice insurance certificate, NPI, CV (5-year work history), government ID, practice TIN, and completed CAQH profile.
Q4: What is the difference between credentialing and provider enrollment?
Credentialing verifies your qualifications. Provider enrollment registers you with payers to obtain billing privileges. Both must be completed before you can receive insurance reimbursement.
Q5: Can I see patients while credentialing is pending?
Yes — but billing is complicated. Some payers allow retroactive billing from your application submission date; others don’t. Confirm each payer’s policy before seeing patients under pending status.
Q6: What is PECOS enrollment for NPs?
PECOS is CMS’s online Medicare provider enrollment system. NPs must complete the CMS-855I application via PECOS to bill Medicare. Processing takes approximately 60–90 days.
Q7: Do telehealth NPs need separate credentialing?
In most cases, yes. Telehealth NPs must be licensed in every state where their patients are located and must complete payer enrollment in each state. Multi-state licensing via the Nurse Licensure Compact (NLC) simplifies licensure in member states, but credentialing requirements remain state-specific.
Q8: What is CAQH and why do I need it?
CAQH ProView is a centralized credentialing database used by most commercial payers. A complete, authorized CAQH profile is required for the majority of commercial payer applications. You must reattest every 120 days to keep your profile active.
Q9: How much does NP credentialing cost?
Per-payer applications run $150–$400. Medicare enrollment: $250–$500. Full-service credentialing packages: $1,200–$3,500 per provider. The cost of delays — typically $20,000–$80,000+ in lost revenue — makes outsourcing a strong ROI.
Q10: How often do NPs need to recredential?
Most payers require recredentialing every 2–3 years. CAQH requires attestation every 120 days. Any changes to your license, malpractice coverage, or practice information require immediate updates to your credentialing records.
Q11: What causes the most common NP credentialing delays?
Incomplete documentation, expired or unauthorized CAQH profiles, incorrect taxonomy codes, mismatched NPI/TIN data, missing collaborative agreements, applying to closed panels, and lack of follow-up with payers.
Q12: Can NP credentialing be done across multiple states simultaneously?
Yes — and for telehealth NPs, it often must be. A professional credentialing service experienced in multi-state NP enrollment can manage simultaneous applications efficiently and ensure state-specific requirements are met in each jurisdiction.
Q13: Can I credential myself as an NP?
Yes, but it requires substantial time, meticulous follow-up, and a solid understanding of payer-specific processes. Most NPs who attempt DIY credentialing underestimate the complexity and end up losing more in delayed revenue than they would have spent on professional services.
Q14: How does credentialing affect NP reimbursement?
Directly and significantly. You cannot bill a payer until your effective participation date. Many payers don’t allow retroactive billing. A 90-day delay in credentialing can mean $20,000–$80,000+ in unrecoverable lost revenue.
Q15: What are the benefits of outsourcing NP credentialing?
Faster approvals, dedicated payer follow-up, reduced admin burden, improved billing readiness, compliance accuracy, multi-state expertise, transparent reporting, and ongoing recredentialing management. Professional credentialing services typically pay for themselves within weeks.
Final Thoughts: Credentialing Is Foundational to Practice Success
Let’s bring it home. Nurse practitioner credentialing isn’t paperwork for paperwork’s sake — it’s the foundation your entire practice revenue is built on. Without proper enrollment and approval:
- Claims cannot be submitted or paid
- Insurance networks cannot be accessed
- Revenue is delayed — often significantly and unrecoverably
- Compliance risks multiply quietly in the background
By understanding the credentialing process, preparing documentation thoroughly, monitoring timelines proactively, and leveraging professional support when needed, NPs can protect their revenue from day one and build sustainable, compliant practices that thrive in 2026 and beyond.
Ready to Get Credentialed? Let TrueCare RCM Handle It.
Credentialing is complicated. It’s time-consuming, error-prone, and the consequences of getting it wrong are expensive. But it doesn’t have to be your problem.
TrueCare RCM LLC is a specialized healthcare credentialing and revenue cycle management company serving nurse practitioners, group practices, and healthcare facilities across 12 states nationwide. We manage the full credentialing lifecycle — CAQH setup, PECOS enrollment, Medicare and Medicaid applications, commercial payer enrollment, and ongoing recredentialing — so you can stay focused on what you went to school for: caring for patients.
Our clients give us a 4.8-star Google rating because we don’t disappear after submitting your application. We follow up with payers, track every application, and keep you informed every step of the way.
States we proudly serve: California, Georgia, North Carolina, Texas, New York, Arizona, Florida, Illinois, Minnesota, Michigan, Maryland, and Virginia.
- Website: https://truecarercm.com/
- Email: info@truecarercm.com
- Phone: (323) 538-6467
Don’t let credentialing delays cost you another week of revenue. Contact TrueCare RCM today — and let’s get you credentialed, enrolled, and billing the right way.
Ready to get credentialed? See our Provider Enrollment & Credentialing Services or learn how Medical Billing & Coding Services can support your entire practice’s revenue cycle.


